πίσω
πίσω
COPYRIGHT © by Michaelidou Maria
Dr. Maria Michailidou
Η General Considerations
Osteoarthritis is the leading cause of arthritis in the adult American population
and affects an estimated 20 million people in the United States. Joint pain is a
frequent symptom that often prompts a patient to seek medical attention, for which
osteoarthritis figures prominently in the differential diagnosis. The challenge for
clinicians is to correctly identify the cause of the patient's pain and to initiate
appropriate therapy, both medicinal and nonmedicinal. Synonymous with degenerative
joint disease, osteoarthritis is characterized by joint pain related to use, the
absence of pain at rest, self-
Characteristic sites of involvement in the peripheral skeleton include the hand (distal interphalangeal joint, proximal interphalangeal [PIP] joint, and first carpometacarpal joint), knee, and hip. Common axial sites with a predilection for osteoarthritis are the lumbar and cervical spine. Constitutional symptoms are characteristically absent. Other than pain or discomfort in the involved joint, the patient with osteoarthritis most often feels well and reports good health.
The diagnosis of osteoarthritis can usually be made relatively easily and confidently based on the history and examination alone. The bedside diagnosis of osteoarthritis can be supported by plain radiography.
Essentials of Diagnosis
Joint pain brought on and exacerbated by activity and relieved with rest. Stiffness
that is self-
Epidemiology
At the population level, osteoarthritis results in substantial morbidity and disability, particularly among the elderly. It is the leading indication for several hundred thousand knee and hip replacement surgeries performed each year in the United States. Therefore, much effort has been invested in improving the understanding of the epidemiology of this disorder, including identifying the factors that predispose persons to osteoarthritis, especially those risk factors that are reversible or modifiable.
Several factors heighten the risk of incident osteoarthritis, including age, gender, and joint injury. While the clinical expression of osteoarthritis begins to manifest during the fourth and fifth decades of life, the incidence of osteoarthritis continues to increase with each decade of aging. Moreover, women in their 50s, 60s, and 70s have a greater prevalence of osteoarthritis in the hand, knee, and hip than do men. There is evidence to suggest that racial differences exist in osteoarthritis prevalence, with greater frequency of knee osteoarthritis in African Americans than in white Americans. Also, prior trauma to a previously pristine joint, such as a ruptured anterior cruciate ligament or torn medial meniscus, increases the risk of later osteoarthritis at that joint site.
Pathogenesis
The pathophysiology of this disorder is related to excessive degradation of cartilage within the involved joint. Elevated production of degradative metalloproteinases, including collagenases, results in tissue breakdown and disruption in assembly of the extracellular matrix. This disruption to the structural integrity of articular cartilage in turn leads to functional compromise of the patient.
Clinical Findings
Symptoms and Signs
The patient with osteoarthritis affecting a joint in the peripheral skeleton, such as the finger, knee, or hip, may initially experience relatively minor pain or discomfort with use of the involved joint ). For example, at the outset of osteoarthritis involving the hip joint, patients may have some difficulty crossing their legs to put on a pair of shoes or pants; however, once they are dressed and upright, bearing weight and ambulation are still well tolerated. As osteoarthritis progresses, a patient will gradually experience progressively severe joint discomfort and increasing difficulty with related activities of daily living.
With further disease progression, such as at an osteoarthritic hand or finger, increasing
difficulty with previously routine activities often follows. Thus, even gripping,
holding, or writing with a pen or pencil can be a painful feat to accomplish. Putting
car keys in and turning the ignition switch, lifting a gallon of milk out of the
refrigerator, or removing a pot of water from the stove can become quite difficult
tasks to accomplish. At this stage, the signs of osteoarthritis joint involvement
include bony enlargement of the involved joint and possibly joint misalignment. At
the extreme end of the disease spectrum, marked impairment in activity follows. Even
walking from room to room in one's home may be unbearably painful when advanced or
end-
Laboratory Findings
There is no specific laboratory test that is used in clinical practice to confirm
a diagnosis of osteoarthritis. Instead, routine laboratory blood testing, including
complete blood cell counts, acute phase reactants (erythrocyte sedimentation rate
and C-
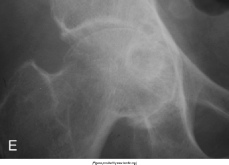
Imaging Studies
Radiographic imaging can confirm the diagnosis of osteoarthritis. More than 4 decades ago, Kellgren and Lawrence described characteristic radiographic features of osteoarthritis—joint space narrowing, osteophytes, subchondral cysts, and bony sclerosis (eburnation). To the present, these parameters remain the radiographic hallmarks of osteoarthritis. While scintigraphy (bone scan) may reveal increased radionuclide uptake at osteoarthritic joints and computed tomography and magnetic resonance imaging may demonstrate characteristic radiographic features of osteoarthritis, these imaging modalities are not routinely used to confirm the diagnosis of osteoarthritis.
Special Tests
Pursuit of a histologic diagnosis via synovial or bone biopsy is not a conventional strategy in the evaluation of a patient with suspected osteoarthritis. However, in the appropriate setting, a joint tap is a valuable test when encountering a patient with presumptive osteoarthritis. When there is subtle—if not moderate evidence—of a mild joint effusion, diagnostic arthrocentesis may be a key aid to confirm the clinical impression. This is because a synovial fluid cell count of 200–2000 cells/L is characteristic of an osteoarthritic effusion; this synovial fluid white blood cell count is intermediate between the upper bound of normal and the lower bound of an inflammatory arthritis.
Differential Diagnosis
The challenge when evaluating a patient with joint pain is to effectively use the history, examination, and available tests to arrive at the correct diagnosis. The presence of pain at the symptomatic joint, brought on by activity and relieved with rest, is quite suggestive of a degenerative arthropathy. Moreover, the absence of constitutional signs and symptoms and the presence of bony enlargement at the joint margin, with little if any evidence of joint inflammation, serve to reinforce this clinical impression. Finally, the pattern of joint involvement is meaningful because primary osteoarthritis has a predilection for particular joint sites in the peripheral skeleton, predominantly the hands (distal interphalangeal joints, PIP joints, first carpometacarpal joint), knees, and hips. The cervical and lumbar spine are preferentially involved sites of involvement in the axial skeleton. These features serve to distinguish osteoarthritis from inflammatory arthropathies (such as rheumatoid arthritis and gout) that have overlapping sites of involvement.
It is also worth noting that a variety of secondary disorders represent identifiable
causes of osteoarthritis. Several such disorders, including those resulting from
inborn errors of metabolism and metabolic derangements. Recognition of their distinct
features, such as predilection for involvement of the second and third metacarpophalangeal
joints in hemochromatosis-
OSTEOARTHRITIS